Since 1993
If you like this strategy for fighting COVID-19, click here to donate to help us work to implement this strategy with our elected and public health officials in the Federal Government and all 50 states.
Our fight against COVID-19 is a war. And COVID-19 is worse than any virus most of us have experienced in our lifetimes: worse than AIDS, Swine Flu, SARS, or MERS. None of these other viruses caused nearly as much death or economic disruption and destruction as our government-led response to COVID-19 has caused.
We must change key aspects of our fundamental approach to COVID-19. Our top public health officials have recommended an approach (and many state governors have imposed it by executive order) that is based on indiscriminate mass lockdowns (except for those whose jobs are designated Essential by the government). This approach is excessively and counter-productively restrictive.
We can safely relax the Stay-At-Home orders and many other restrictions IMMEDIATELY if we shift our primary focus...
⦁ Away from trying to reduce the number of infections/cases for everyone, and..
⦁ Toward protecting those at higher risk of death: those with Pre-Existing Medical Conditions (PEMCs) such as hypertension, diabetes, lung and cardiac disease, immunodeficiency, asthma, kidney disease, cancer, and gastro-intestinal/liver disease. ..
⦁ These pre-existing conditions are much more important risk factors than age alone.
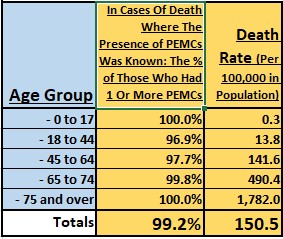 Data from New York City (NYC) [see the graphic to the right with data as of May 9th], shows that those who died from COVID-19 AND for whom their Pre-Existing Medical Condition status was known, about 99.2% had one or more of those conditions. Consequently, COVID-19 is not a significant threat to people who are not afflicted by those conditions, which is the vast majority of students and working-age people. NYC is one of the few places that has tracked COVID-19 deaths by Pre-Existing Medical Conditions. But, there is no reason to believe that that percentage (or something close to it) is not applicable to the rest of the country, even though the population death rates are substantially different.
Data from New York City (NYC) [see the graphic to the right with data as of May 9th], shows that those who died from COVID-19 AND for whom their Pre-Existing Medical Condition status was known, about 99.2% had one or more of those conditions. Consequently, COVID-19 is not a significant threat to people who are not afflicted by those conditions, which is the vast majority of students and working-age people. NYC is one of the few places that has tracked COVID-19 deaths by Pre-Existing Medical Conditions. But, there is no reason to believe that that percentage (or something close to it) is not applicable to the rest of the country, even though the population death rates are substantially different.
Therefore, we can safely and immediately replace our current, excessively restrictive, approach with a targeted strategy[1] based on the different risks that people face. Based on their medical conditions, people would categorize themselves as being in either...
⦁ The Higher Risk Group (those with those pre-existing medical conditions regardless of age, but who also tend to be more elderly) should largely continue to voluntarily self-isolate (not because of government mandates), and
⦁ The Very Low Risk Group (those without those pre-existing medical conditions) can safely and should immediately go back to work and fully participate in the economy, so that we can stop the economic destruction of our country.
⦁ Adopt a freedom and risk-based strategy that gives individual citizen comprehensive, accurate information about the risks they face.
⦁ Trust individual citizens make free decisions about how they live, work, and play.
⦁ Make treatment options a central part of our strategy. Options such as:
⦁ Hydroxychloroquine with Azithromycin early enough and in high enough dosages.
⦁ Anti-body containing blood plasma from those who have been infected and recovered (Convalescent blood plasma).
⦁ Enables businesses not to just reopen, but to reopen without drastic, unprofitable changes to their operating models. Examples:
⦁ Sit-down restaurants would not need a 6-foot separation between ALL tables, which is not profitable for most. Instead:
⦁ They could have that 6-foot separation in a small section for the fairly small minority of patrons who are at high-risk,
⦁ Use their traditional (profitable) table separation in most of their dining area for patrons in the vast, low-risk majority,
⦁ And/or have separate hours for their high-risk and low risk customers.
⦁ Office-based businesses could use a similar strategy: require 6-foot social distancing only for employees who are at high-risk.
⦁ Does not depend on large-scale testing to determine who is or has been infected (which is not feasible any time soon)
⦁ Also, does not require contract tracing which would have been valuable very early in the epidemic, but not now.
⦁ Success can be monitored through weekly hospitalization counts, which are much more reliable over time than case counts as an indicator of progress against COVID-19.
[1] These statistical conclusions are also endorsed by Dr. Scott Atlas, former chief of neuroradiology at Stanford University in an article titled The Data Is In — Stop The Panic And End The Total Isolation.
Next Steps...
- Evaluate on-line Quick Summary of Vertex Decisions' strategy for resolving the COVID-19 crisis.
- Send an email asking for more information about Vertex Decisions' strategy for resolving the COVID-19 crisis.
- Or, read about Vertex Decisions' data architecture and data analytics offerings.